- Home
- POMA
- POMA Foundation
- DO Voices
- Residents & Students
- Resident Information
- Student Information
- Scholarship Opportunities
- Clinical Writing Contest
- Scientific Poster Session
- Winter Residency Fair
- Education
- Advocacy
- Affiliates
- Public
|
Adrenaline Rush: A Ruptured Pheochromocytoma Masquerading as Abdominal Pain June 2026 | Vol. 70, No. 2 ABSTRACT INTRODUCTION CASE REPORT A 45 year old male presented to our ED after being seen at a local urgent care for sudden onset left-sided abdominal pain. On arrival to the ED the patient was tachycardic to the 120-130s bpm and hypertensive at 226/118. He reported associated nausea, vomiting and lightheadedness. During the initial physical exam the patient was noted to be diaphoretic and appeared to be in acute distress. The abdominal exam showed tenderness and guarding with palpation of the left upper quadrant. Bowel sounds were present and normal. There was no abdominal distension. There were no rashes, ecchymosis, or signs of trauma. 1 Sunga et al., 2012 https://www.jem-journal.com/article/S0736-4679(11)00626-3/fulltext Computed tomography (CT) of the abdomen and pelvis was performed with intravenous (IV) and oral contrast revealing acute retroperitoneal hematoma with active extravasation. During this time the patient remained severely hypertensive and tachycardic despite pain management with IV hydromorphone. Interventional Radiology (IR) was emergently consulted and reviewed the CT images. IR identified extravasation from the region of the adrenal gland. The patient was treated for suspected adrenal gland hemorrhage and possible catecholamine surge with primary concern for ruptured pheochromocytoma. Accordingly, beta blockade was avoided and the patient was started on a nicardipine infusion. The patient was taken to the embolization suite where active extravasation was noted from the left adrenal artery arising from the left lower pole renal artery. Gelfoam embolization was successfully completed by an IR physician and the patient was subsequently admitted to the Intensive Care Unit (ICU). Further workup in the ICU revealed elevated serum normetanephrine (NMN) at 268 pg/mL as well as an elevation in the total free (Metanephrine + NMN) at 319 pg/mL. These levels, though elevated, were in an indeterminate range, though given the patient’s presentation ruptured pheochromocytoma was suspected. The patient was ultimately discharged from the hospital in stable condition with instructions to follow up
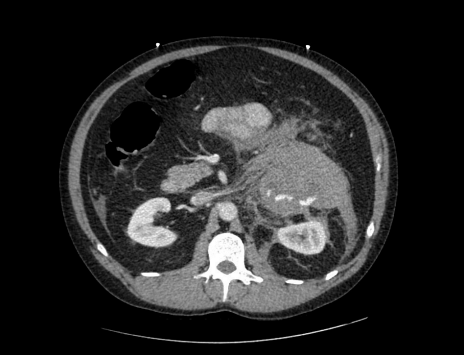
Image 1. Computed tomography (CT) of the abdomen and pelvis with intravenous contrast in the coronal view showing area of hemorrhage superior to the left kidney
Image 2. Computed tomography (CT) of the abdomen and pelvis with intravenous contrast in the sagittal view with active extravasation DISCUSSION SRH due to ruptured pheochromocytoma is a rare yet critical emergency. Patients often present with nonspecific symptoms that can delay diagnosis and definitive treatment. This case highlights a triad of abdominal pain, hemodynamic instability and hypertension which should raise suspicion for catecholamine secreting tumors. While most pheochromocytomas are diagnosed in a controlled outpatient setting based on classic symptoms such as episodic hypertension, headaches, diaphoresis, and palpitations, rupture with hemorrhage is an uncommon and life-threatening presentation. Imaging played a key role in identifying the SRH and localizing the source of bleeding. In our case, CT demonstrated active retroperitoneal hemorrhage with a suspected pheochromocytoma as the origin. Biochemical testing post-embolization showed elevated normetanephrine and total catecholamines, supporting the suspicion of a pheochromocytoma. It is notable that these levels were only moderately elevated, possibly influenced by the acute hemorrhagic state or stress response. Repeat biochemical evaluation and subsequent imaging (e.g., MRI or MIBG scintigraphy) are essential for confirming diagnosis and guiding long-term management, including surgical resection once the patient is stabilized. Sympathetic surge related to suspected pheochromocytoma rupture should be managed with IV anti-hypertensives, though very close monitoring is required as hemorrhage may result in subsequent hypotension. Beta-blockade without alpha-blockade can precipitate unopposed alpha-adrenergic activity, leading to worsening hypertension or circulatory collapse. In this instance, the use of nicardipine—a calcium channel blocker—was sufficient for acute blood pressure control. Ultimately, this case emphasizes the need for high clinical suspicion and rapid multidisciplinary intervention in cases of SRH. Emergency physicians, radiologists, intensivists, and endocrinologists collaborated to stabilize the patient, confirm the diagnosis, and provide definitive treatment. Awareness of pheochromocytoma as a rare but serious cause of SRH can lead to improved patient outcomes through timely intervention. References 1. Kobayashi, T., Iwai, A., Takahashi, R., Ide, Y., Nishizawa, K., & Mitsumori, K. (2005). Spontaneous rupture of adrenal pheochromocytoma: Review and analysis of Prognostic Factors. Journal of Surgical Oncology, 90(1), 31–35. doi:10.1002/jso.20234 2. Souiki, T., Tekni, Z., Laachach, H., Bennani, A., Zrihni, Y., Tadmori, A., … Aitlaalim, S. (2014). Catastrophic hemorrhage of adrenal pheochromocytoma following thrombolysis for acute myocardial infarction: Case report and literature review. World Journal of Emergency Surgery, 9(1). doi:10.1186/1749-7922-9-50 3. Sunga, K. L., Bellolio, M. F., Gilmore, R. M., & Cabrera, D. (2012). Spontaneous retroperitoneal hematoma: Etiology, characteristics, management, and outcome. The Journal of Emergency Medicine, 43(2). doi:10.1016/j.jemermed.2011.06.006 |